- By shoulderadm
- In Blog
Ac joint dislocation
AC JOINT DISLOCATION
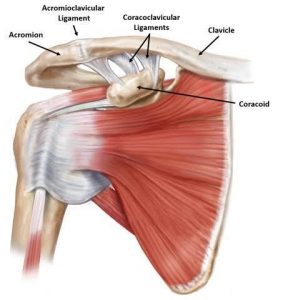
Anatomy and biomechanics
- Diarthoidal joint – plane type of synovial joint
- Superior capsule blended with deltoid and trepizius
- supero inferior and antero posterior movents
- Fibrous capsule
Typical features
- Cartilage – fibrocartilage
- Joint partially devided by articular disc.

Ligaments
- AC ligament :
- horizontal stabilizer
- Resist 90% of A-P translation and joint distraction
- Posterior and superior AC capsular ligaments provide greatest stability
- Clinical importance of distal clavicale resection
- CC ligament :
- vertical stabilizer
- Conoid– primary restraint to superior translation
- Trepizoid resists 75% of AC joint compressionz
- Fukuda et al.,jbjs 1986; klimkiewicz et al.,jses 1999
- Conoid– attaches posterior and medial on clavicle
- 2ndligament to fail after ac ligament
- Trepizoid– attaches anterior and lateral on clavicle
- Movements : ac joint have passive movements with coordination of scapular movements
- 5 to8 deg of movement present during elevation of arm above 90deg

Mechanism of injury
Direct
- Most common
- Direct force to acromion with shoulder adducted only
- Acromion is moves inferiorly and medially (clavicle stabilized by sc joint)
Indirect
- Less common
- Out stretched hand
- Typically affects AC ligaments
Order of failure –
- ac ligaments/capsule
- CC ligaments
- Deltotrapezial fascia
Diagnosis
Clinical :
- tenderness over lateral end of clavicle or shouler
- swelling or deformity
- Stability of joint and reducible or not
- Special tests – O Brein‘s active compression test. Paxinos sign cross body addiction test and resisted extension test
- Sc joint and neurological examination
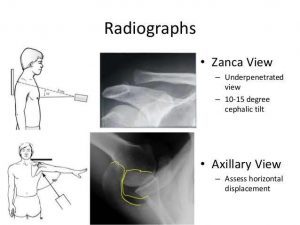
Imaging :
- X ray : AP view Stress view zanca view – specific and sensitive for ac joint Axillary view – ap translation
- Ct/mri– rare suspected other injuries
 Classification
Classification
- Mainly based on vertical and horizontal instability
- Allman (Allman F L, JBJS (am) 49:774-784, 1967)
- Tossyet al – (Tossy et al, CORR, 28: 111-119, 1963)
- Later modified by Rockwood(In: Fractures in adults, edited by Rockwood, CA, 1341-1414, Lippincott-Raven, 1996)


Management

Reid et al 2012 – conservative management is the main recommendation for grades 1-3

Conservative management
Gladstone protocol (1997)
pain relief and protection
Phase 2 – ROM and early isotonic strengthening
Phase 3- advanced strengthening and dynamic AC joint stability strengthening
Phase 4– sports specific training
Rehabilitation
- Early focus is on passive and active ROM
- Once symmetric and painless ROM achieved then progress to isometric shoulder strengthening
- Isotonic strengthening
- Sport specific training
- Return to sports by 2-3months
Surgical management
- For type IV and above
- Methods :
- Fixation across AC joint
- Fixation between coracoid and clavicle
- Ligament repair +/- augmentation or fixation
- Anatomical Ligament reconstruction
- Distal clavicle excision
Phemister technique
-
- Recently not used alone because of complications
- Used with other procedures to augment them
- Complications-
- Pin breakage and migration
- Recurrence of lesion

Hook plate
-
- Only used for acute cases
- Requires subsequent removal
- Osteolysis – 17%
- Protrusion and irritation of skin


Bosworth technique

Mazzocca et al, AJSM 2007
-
- Cadaveric study
- Distance between lateral end of clavicle to conoid tuberosity : 45mm
- To trapezoid tuberosity : 25mm

Tight rope
-
- Instead of screw using tight rope with endobuttons
- Used along with the repair of ligaments to augment

Ligament reconstruction

-
- Resection of distal clavicle incresar the horizontal translation so it should be graded and determental
- Intact of distal clavicle decreases the force on postero superior aspect of AC ligaments

-
- Results: There were significant increases in AP translation with the cut AC joint capsule, and significant increases in SI translation with the cut CC ligaments (P < 0.0001). Compression significantly decreased translation (P < 0.0001).
- To conclude
- Distal clavicle resection is determental but
- Ac ligament and capule repair or re construction gives good results
Waver Dunn procedure
-
- Distal clavicle excision
- The ca ligament is transferred to the distal clavicle
- CC ligaments are repaired +/augmentation
- Repair of deltotrapezial fascia
- Ac joint not addressed

Mazzocca technique
-
- Campell describes
- Anatomic reconstruction of cc ligaments

Anatomical reconstruction
- Grafts :autigrafs (hamstrings)
- Allografts :
- LARS
- SURGILIG
- RotaLok system
- Keio Leeds system

LARS
- Braided polyethylenetraphthalate
- 100N tensile strength
- Vascularisation and fibrous ingrowth – type I collagen
- Failure may be due to malposition of tunnels in the clavicle
- Anatomic reconstruction has higher loads of failure



Newer techniques
- Gritter and Petersen technique




Complications of ac joint dislocation
- Arthritis
- Cosmetic
- Scapular dyskinesia
- Sick scapula syndrome
- Shoulder weakness and stiffness
- Rotator cuff problems
Sick scapula syndrome
- Scapular malposition
- Inferomedial prominence of scapula
- Coracoid pain and Kinesial abnormalities of scapula




