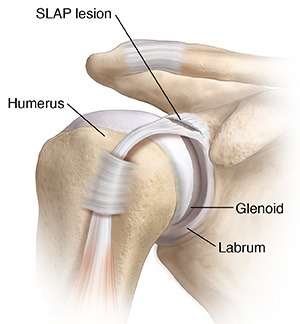
SLAP is an acronym that stands for Superior Labral Tear from Anterior to Posterior. A SLAP tear is also referred to as a labral Tear or SLAP Lesion. It is an injury to the labrum of the shoulder. As we know, the shoulder is a ball and socket joint. The labrum is a cartilage lining around the socket of the shoulder. The labrum helps to deepen the socket and stabilize the shoulder joint. SLAP lesion is a damage to the top of the labrum, or where the biceps tendon connects to the labrum. A SLAP tear occurs both in front (anterior) and back (posterior) of this attachment. Depending on the type of injury, the SLAP tears are classified into several types:
SLAP Tear
SLAP Tear
Types of SLAP Tear
There are several types of Slap Tears:
Type 1 SLAP Tear
Involves isolated fraying of the labrum, but it is still attached to the Glenoid. Generally, does not show any symptoms. It is said that most of the people have a Type 1 SLAP tear that they would not know of.
Type 2 SLAP Tear
This is the most common type of SLAP Tear. Involves detachment of labrum from the Glenoid causing instability of the biceps-labral anchor. They can be further classified as anterior, posterior or a blend of the two.
Type 3 SLAP Tear
Involves bucket-handle tear of the labrum. Biceps anchor are attached. Labrum droops into the shoulder joint. Often treated with Arthroscopy
Type 4 SLAP Tear
This is again a bucket-handle tear of the labrum however it extends upto the biceps tendon in varying degrees. It also involves instability of the biceps-labrum anchor. Depending on the extent of biceps tendon involved, treatment options are selected.
Causes of SLAP Tear
SLAP tears are generally caused by repeated motions or acute trauma. Athletes have high chances of getting a SLAP tear. The main causes are:
Due to an injury – fall or sudden force
Wear and tear due to age
Repeated overhead motions like in volleyball, swimming
Lifting heavy objects too often or suddenly
Symptoms of SLAP Lesion
Pain with specific movements of shoulder.
Decreased strength in the shoulder
Limited range of motion
Popping, clicking or catching sensation in the shoulder
Inflammation in the shoulder
Diagnosing a shoulder labral tear
A Shoulder Specialist will evaluate the patient’s medical history which includes discussing the symptoms, current occupation, previous treatments, medications etc. Evaluating medical history of the patient along with physical examination plays a very important and intricate part of diagnosing the problem. In many cases, doctor diagnoses the problem based on medical history and physical examination which is then validated using x-rays or imaging technologies.
Treatment of SLAP Tear
Like other shoulder conditions, treatment starts with the following standard non-surgical methods:
Non-steroidal anti-inflammatory medications
Physical Therapy
If the symptoms persist even after taking standard non-surgical treatment for a considerable period of time, based on the case a surgery will be recommended.
Surgical Treatment
Arthroscopy
The technique commonly used to correct a SLAP tear is shoulder arthroscopy where very small incisions are made in the shoulder. Best repair option through arthroscopy is determined depending on the type of SLAP tear a patient has.
Rehabilitation
Depending on the severity of the SLAP injury, a sling will be recommended for a particular duration. Once the pain and swelling subsides, doctor will recommend customized physical therapy sessions. The aim is to regain the strength of the shoulder and resume normal shoulder functions.
For enquiries and online appointments, send message to www.BangaloreShoulderInstitute.com/contact
Q&As on SLAP Tear
1. Why are SLAP tears often difficult to diagnose?
SLAP tears can be challenging to diagnose because their symptoms overlap with those of other shoulder conditions. Pain location is often vague, and physical examination tests are not always definitive. Many patients report deep pain, clicking, or weakness, which can also occur with rotator cuff or biceps problems.
Imaging helps, but a standard MRI does not always show the tear clearly. Even advanced scans must be interpreted alongside symptoms and examination findings. Some labral changes are also seen in people without pain, especially as they age, which complicates diagnosis.
For this reason, diagnosis is based on a combination of history, examination, imaging, and treatment response rather than on a single test result. Careful assessment prevents unnecessary procedures and guides appropriate management.
2. Can a SLAP tear improve without surgery?
Yes, many SLAP tears can be managed without surgery, particularly when symptoms are mild or activity demands are lower. Non-surgical treatment focuses on reducing inflammation, restoring shoulder movement, and improving muscle balance around the joint.
Physiotherapy aims to stabilise the shoulder blade, improve rotator cuff function, and reduce stress on the labrum. Activity modification plays an important role, especially avoiding movements that aggravate symptoms during early recovery.
Improvement depends on factors such as age, activity level, and associated shoulder problems. While the tear itself may not heal anatomically, symptoms often settle enough to allow comfortable function. Surgery is considered only when symptoms persist despite appropriate rehabilitation.
3. Why does age influence treatment decisions for SLAP tears?
Age affects both shoulder biology and response to treatment. In younger individuals, the labrum and biceps tendon are often healthier, increasing the likelihood of successful repair. In older patients, the labrum is often degenerative, and repair may lead to stiffness or persistent pain.
With increasing age, the biceps tendon itself often becomes a source of pain. In such cases, addressing the biceps rather than repairing the labrum may provide better symptom relief. Age also influences recovery expectations and risk of complications.
Therefore, treatment is tailored to the individual rather than the tear type alone. The goal is reliable pain relief and function, not simply fixing what appears abnormal on imaging.
4. How do SLAP tears affect return to work or sport?
Return to activity after a SLAP tear varies widely. Every day, work activities often resume earlier than high-demand or overhead tasks. Jobs involving lifting, repetitive arm use, or sustained overhead positions may take longer to tolerate comfortably.
Return to sport depends on the sport type, level, and treatment approach. Overhead sports place higher stress on the superior labrum, making return less predictable. Rehabilitation focuses on restoring strength, control, and confidence rather than speed alone.
Setting realistic expectations is important. A successful outcome means pain-free, functional use of the shoulder rather than guaranteed return to the previous performance level in all cases.
5. Why is individualised treatment planning so important for SLAP tears?
SLAP tears are not all the same, even when labelled similarly. Tear pattern, shoulder anatomy, muscle balance, age, and activity demands all influence outcome. Associated problems, such as rotator cuff pathology or joint stiffness, also affect treatment choice.
A standard approach does not work for everyone. Some patients do best with rehabilitation alone, others benefit from addressing the biceps, and a smaller group require labral repair. Choosing the wrong strategy can lead to prolonged symptoms or revision surgery.
Individualised planning focuses on the person, not just the diagnosis. This approach improves satisfaction, reduces complications, and supports long-term shoulder health.
6. Can a SLAP tear cause shoulder weakness?
Yes. Pain and altered movement can reduce muscle activation, leading to functional weakness. This is usually reversible with proper rehabilitation once pain and control improve.
7. Why do some people feel worse after SLAP surgery even when the repair looks successful?
A technically successful repair does not always translate into symptom relief. The shoulder is a finely balanced joint, and tightening one structure can alter how forces are shared across others. In some patients, especially those with pre-existing stiffness or muscle imbalance, repairing the labrum can reduce the joint’s natural adaptability.
Post-surgical pain may also come from the biceps tendon or surrounding tissues rather than the labrum itself. If these contributors are not addressed, symptoms can persist. This is why the outcome depends not only on what is repaired, but on whether the repair matches the patient’s shoulder mechanics and daily demands.
8. Why do surgeons sometimes recommend not repairing the torn labrum at all?
In some cases, the labrum tear is not the main source of pain. Degenerative labral changes are common with age and may be present even in people without symptoms. Repairing such tissue can add stiffness without solving the problem.
In these situations, treatment may focus on reducing stress through the biceps tendon or improving shoulder mechanics instead of restoring anatomy. The aim is symptom relief and function, not cosmetic repair. Avoiding unnecessary repair can lead to better comfort and faster recovery in selected patients.
9. Why is recovery after SLAP surgery more unpredictable than other shoulder procedures?
The superior labrum plays a role in stability, motion, and load sharing. Healing alters how these forces interact, particularly during overhead or pulling activities. Unlike procedures with a single mechanical goal, SLAP surgery affects multiple systems at once.
Recovery depends heavily on how well the shoulder adapts to these changes. Factors such as age, work demands, movement habits, and rehabilitation quality influence outcome more than the tear type alone. This explains why two patients with similar scans can have very different recoveries.
10. How do daily work demands influence surgical decision-making more than sports level?
While sports often get attention, many shoulders fail under repetitive work rather than athletic load. Tasks such as lifting, pushing, sustained reaching, or working at shoulder height place continuous stress on the superior labrum and biceps.
If surgery does not account for these demands, symptoms may persist despite good healing. Therefore, understanding how the shoulder is used at work is often more important than whether someone plays sports. Treatment is planned around real-world load, not labels like ‘athlete’ or ‘non-athlete’.
© Copyright 2025 Bangalore Shoulder Institute