- By shoulderadm
- In Uncategorized
KNEE JOINT INJURIES
ACL INJURY:
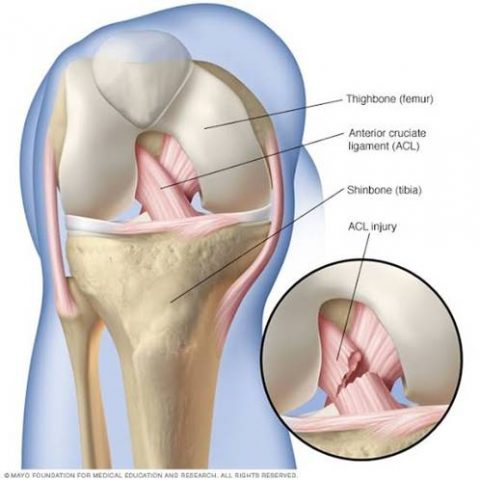 The knee joint is the most commonly injured of all joints and the anterior cruciate ligament (ACL) is the most commonly injured ligament
The knee joint is the most commonly injured of all joints and the anterior cruciate ligament (ACL) is the most commonly injured ligament
Anatomy:
ACL attaches at lateral femoral condyle and posterior to anterior horn of medial meniscus
ACL has two bundles: anteromedial and posterolateral
Functions of ACL:
The ACL functions in concert with all other anatomical structures in and around the knee joint to control and limit the motion and to maintain both static and dynamic equilibrium.
ACL has two complementary roles:
- Proprioception
- Mechanical –
- The ACL, principally the anteromedial band accounts for the resistance to anterior tibial translation on the femur with the knee in 90* flexion.
- The posterolateral portion provides the principal re-sistance to hyperextension.
- It provides a check to internal axial rotation and thereby affords rotatory control of the knee.
- It is a secondary restraint resisting both valgus and varus strains in all degrees of flexion.
- Tension in the ACL fine tunes the ‘SCREW HOME’ movement stabilizing the joint as it approaches terminal extension.
Causes of injury: pivoting and twisting injuries
Symptoms:
Recurrent episodes of instability, pain and decreased function.
Diagnosis:
Clinical evaluation: Lachman test
Anterior drawer test
XRAY: avulsion injuries and Segond’s fracture
MRI: complete evaluation of ACL
- Partial tear
- Complete tear
Treatment:
Immediate – Rest, Ice, Immobilisation
Later – depends on tear
- Conservative: brace application
Lifestyle modification
Physiotherapy
- Operative: arthroscopic reconstruction with hamstring graft or BTBP graft
Fixation: Endobutton and interference screw
PCL/ POSTERIOR CRUCIATE LIGAMENT INJURY:
 ANATOMY –
ANATOMY –
The posterior cruciate ligament (or PCL) is one of the four major ligaments of the knee. It connects the posterior intercondylar area of the tibia to the medial condyle of the femur.
- The PCL is a strong fan shaped and intracapsular ligament along with the anterior cruciate ligament (ACL). • They are both isolated from the fluid-filled synovial cavity, with the synovial membrane wrapped around them.
- It has two parts a. Anterolateral b. posteromedial
Function :
The function of the PCL is to prevent the femur from sliding off the anterior edge of the tibia.
- Prevents hyperflexion of the knee to a lessor extent with ACL but its main function is to check extension and hyperextension.
- It also helps in checking the rotational movements with ACL.
Mechanism of injury –
- Direct blow to the knee while it is flexed(dashboard injury)
- Falling hard on the knee
- Hyperextension Injury • (Any Mechanism That Involves The Knee To Be Forced Posteriorly Can Leads To Pcl Injury).
Diagnosis:
History
- Special tests – Posterior drawers test
- Reverse lachmans test
- Godfreys test
- x – ray/M.R.I/C.T scan
Treatment :
- Complete rest -supportive brace for grade 1 and grade 2 tear of PCL
- Surgical intervention – Surgery is performed for grade 3 and grade 4 tearing.
- Graft is taken from either hamstrings or achilles tendon.
- Ligament reconstruction arthroscopy is performed
MENISCUS INJURY:
 Menisci are crescentic fibro cartilaginous structures between femoral condyles and tibia
Menisci are crescentic fibro cartilaginous structures between femoral condyles and tibia
They are tibial extension that creates conformity b/w the relatively flat tibial surface and round femoral
condyles
- Made up of type 1 collagen with some type 2 and some elastin fibers
FUNCTIONS OF MENISCI
- Joint lubrication
- Joint stability- ( rotary)
- Joint nutrition Shock absorbers-reduce the stress on articular cartilage
- Load bearing function
- Deepening the cavity
Pedisposing Factors
- Trauma
- Meniscal cyst
- Decreased mobility of the meniscus
- Discoid meniscus
- Aging- degeneration
- Abnormal mechanical axis- ligamentous laxity.
Mechanism of injury-
Rotational force when a flexed knee extends
Twisting strain when knee is flexed;
Young active athletes are more prone (An acute twisting injury from impact during a sport)
In middle aged: fibrosis decreases the mobility and hence tear occurs with less force
Getting up from a squatting or crouching Position.
Symptoms –
- Not all meniscal tears are symptomatic
- Swelling
- Pain along the joint line (tenderness)
- Pain when squatting, kneeling or pivoting
- Locking of the knee
- Giving way snaps, clicks, catches in knee.
- Atrophy of quadriceps
- Instability of joint
Diagnosis –
History
Special tests –
- McMURRAY’S TEST
- APLEY’S GRINDING TEST
- SQUATT TEST
- STEIAMNN TEST
- KNEE JERK TEST
Diagnosis –
MRI:
Is currently of great value in the diagnostic evaluation of meniscal tears.
The accuracy of meniscal tears exceeds 90%.
Arthroscopy: it has accuracy about 95 -98%
Initial Treatment –
Initial treatment of a meniscal tear follows the basic
RICE formula: rest, ice, compression and elevation, combined ith nonsteroidal anti-inflammatory
Medications for pain.
NON SURGICAL TREATMENT:
Indication:
- Incomplete meniscal tear or small (5mm) stable peripheral tear with no pathological condition.
- Tears associated with ligamentous instabilities can be treated nonsurgically
If patient defers ligament reconstruction or if reconstruction is contraindicated
Treatment –
- Immediate abstinence from weight bearing, rest with knee flexion, application of ice packs and compression dressing.
- Traction with 5 to 7 pounds of weight.
- Fluid should be aspirated.
- A single intra-articular steroid injection should be permissible.
- Squatting, flexion, external rotation and valgus stress to the knee to be avoided in the first week.
- Groin to ankle cylindrical cast to be worn for 4 to 6 weeks.
- Isometric exercise program during the time the leg is in cast.
- At 4 to 6 weeks cast is removed and rehabilitative program is intensified.
- 10.If symptoms recur after a period of NST, surgical repair or removal of damaged meniscus may be necessary.
SURGICAL TREATMENT –
ARTHROSCOPIC MENISCECTOMY – PARTIAL / SUB TOTAL/TOTAL
- Narrowing of joint space
- Flattening and squaring of femoral condyle
- Antero posterior osteophyte formation (ARTHRITIS)
ARTHROSCOPIC MENISCALL REPAIR –
- ALL INSIDE TECHNIQUE
- INSIDE OUT TECHNIQUE
- OUTSIDE IN TECHNIQUE
MCL /MEDIAL COLLATERAL LIGAMENT INJURIES:
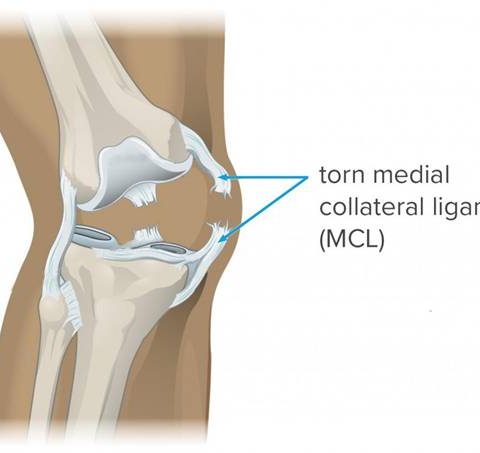 The medial collateral ligament (MCL) is a flat band of connective tissue that runs from the medial epicondyle of the femur to the medial condyle of the tibia and is one of four major ligaments that supports the knee
The medial collateral ligament (MCL) is a flat band of connective tissue that runs from the medial epicondyle of the femur to the medial condyle of the tibia and is one of four major ligaments that supports the knee
This structure is divided into superficial and deep ligaments.
FUNCTION –
- Valgus stabilisation
- Prevents anterior translation of tibia
- Rotational stability
MECHANISM OF INJURY –
- Direct blow on lateral aspect
- Valgus stress
- Forced external rotation
Symptoms – Swelling, Pain, Locking and Instability
Diagnosis –
History
Tests – valgus stress test at 0 and 30 deg flexion
Investigations: x ray / MRI
Treatment –
Non operative – Rest
Bracing
Physiotherapy
Operative: Open / Arthroscopic repair
Reconstruction of MCL ligament with graft
Rehabilitation:
Protective weight bearing with brace
0 – 90 deg for 2 weeks
Full flexion by 6 weeks
Remove brace after 6 weeks
Strengthening of quadriceps and hamstrings
Avoid pivoting for 16 weeeks
Jogging 16 -20 weeks
Sports – 9 months
LCL/ LATERAL COLLATERAL LIGAMENT INJURY:
 Lcl is extra articular collateral ligament attaches at lateral condyle of femur and at fibular head
Lcl is extra articular collateral ligament attaches at lateral condyle of femur and at fibular head
Functions –
Primary stabilizer to varus stress
Resistance to external rotation
Mechanism of injury –
Varus and hyperextension injuries
Diagnosis :
History
Tests – varus stress test
External rotation and recurvatum test
Investigations –
X ray – stress views
Avulsion fractures
MRI
Treatment –
Conservative – For grade one and grade two injuries
Immobilisation with brace
Physiotherapy
Operative: Complete tear or avulsion injuries
Repair or reconstruction
PATELLAR DISLOCATIONS:
 Patella is largest sesmoid bone in body. It articulates with femur and forms patellofemoral joint.
Patella is largest sesmoid bone in body. It articulates with femur and forms patellofemoral joint.
Patellar dislocation means patella moved away from the trochlear groove.
Causes:
- Soft tissue – Mpfl deficiency and VMO weakness
Lateral retinaculum and ITB contracture
- BONY – Patella alta
Trochlear dysplasia
- Lowe limb malalignment – Genu valgus
External tibial torsion
Increasesd Q angle
- Gait abnormalities
- Trauma
Mechanism of injury:
Direct injury –rare
Indirect injury: forceful contraction of quadriceps contraction while knee in flexion, valgus and external rotation position
Types of dislocation:
- Acute dislocation
- Recurrent dislocation
- Habitual dislocation
Symptoms: Swelling, Pain and Restricted ROM
Diagnosis:
History
Tests:
- Patellar grinding test
- Patellar tacking
- Patellar tilting
- Quadrant test
- Apprehension test
- Q Angle
Investigation –
X ray –
- Ap and lateral view
- Skyline view
- Laurin view
- Axial view
CT scan
MRI
TREATMENT:
Conservative –
- Rest, ice application and immobilization for 4-6 weeks
- Cylindrical cast or brace applied
- McConnell taping
- Quadriceps training (VMO)
- Bare foot running
Operative:
Depends on cause
- Mpfl reconstruction
- Lateral retinacular release
- Medial retinaculum tightening
- Trochlear depth increasing by osteotomy
- Tibial tubercle osteotomy and transfer
Rehabilitation:
CARTILAGE INJURIES:
Anatomy:
Articular cartilage has extraordinary mechanical properties and lasting durability even though it is only a few millimeters thick. Its unique structure and composition provides joints with a surface that combines low friction with high lubrication, shock absorption, and wear resistance while bearing large repetitive loads throughout a person’s lifetime.
Articular cartilage: mostly hyaline cartilage
Causes: repetitive loads because of malalignment
- Trauma
- Aging (wearing)
- Osteochondritis Dessicans
Evolution: history , physical examination
MRI: Cartilage mapping
Arthroscopic
Classification
Management:
- Physiotherapy
- Life style changing
Surgical: Arthroscopic drilling (microfracturing)
- BMAC (bone marrow)
- ACI
RUNNER’S KNEE :
Runner’s knee is the common term used to describe any one of several conditions that cause pain around the kneecap, also known as the patella. These conditions include anterior knee pain syndrome, patellofemoral malalignment, chondromalacia patella, and iliotibial band syndrome.
As the name suggests, running is a common cause of runner’s knee, but any activity that repeatedly stresses the knee joint can cause the disorder. This can include walking, skiing, biking, jumping, cycling, and playing soccer.
runner’s knee is more common in women than in men, particularly in women of middle age. People who are overweight are especially prone to the disorder.
Symptoms:
The hallmark of runner’s knee is a dull, aching pain around or behind the kneecap, or patella, especially where it meets the lower part of the thighbone or femur.
You may feel pain when:
- Walking
- Climbing or descending stairs
- Squatting
- Kneeling
- Running
- Sitting down or standing up
- Sitting for a long time with the knee bent
Other symptoms include swelling and popping or grinding in the knee.
In the case of iliotibial band syndrome, the pain is most acute on the outside of the knee. This is where the iliotibial band, which runs from the hip to the lower leg, connects to the tibia, or the thicker, inner bone of the lower leg.
Causes:
The pain of runner’s knee may be caused by irritation of the soft tissues or lining of the knee, worn or torn cartilage, or strained tendons. Any of the following can also contribute to runner’s knee:
- Overuse
- Trauma to the kneecap
- Misalignment of the kneecap
- Complete or partial dislocation of the kneecap
- Flat feet
- Weak or tight thigh muscles
- Inadequate stretching before exercise
- Arthritis
- A fractured kneecap
- Plica syndrome or synovial Plica syndrome, in which the lining of the joint becomes thickened and inflamed
In some cases, pain begins in the back or hip and is transmitted to the knee. This is known as “referred pain.”
Diagnosis:
To confirm a diagnosis of runner’s knee, your doctor will obtain a complete history and conduct a thorough physical examination that may include a blood test, X-rays, an MRI scan, or a CT scan.
Treatment:
Your doctor will tailor your treatment to the underlying cause, but in most cases, runner’s knee can be successfully treated without surgery. Most often, the first step in treatment is to practice RICE:
- Rest: Avoid repetitive stress on the knee.
- Ice: To reduce pain and swelling, apply an ice pack or a package of frozen peas to the knee for up to 30 minutes at a time and avoid any heat to the knee.
- Compression: Wrap your knee with an elastic bandage or sleeve to restrict swelling but not too tightly as to cause swelling below the knee.
- Elevation: Place a pillow under your knee when sitting or lying down to prevent further swelling. When there is significant swelling, keep the foot elevated above the knee and the knee above the level of the heart.
If you need additional pain relief, you can take certain over-the-counter nonsteroidal anti-inflammatory medications (NSAIDs).
Once the pain and swelling has subsided, your doctor may recommend specific exercises or physical therapy to restore your knee’s full strength and range of motion. They may tape your knee or give you a brace to provide extra support and pain relief. You may also need to wear shoe inserts known as orthotics.
Surgery may be recommended if your cartilage is damaged or if your kneecap needs to be realigned.
Prevention:
The American Academy of Orthopaedic Surgeons recommends the following steps to prevent runner’s knee:
- Stay in shape. Make sure your overall health and conditioning are good..
- Do a five-minute warmup followed by stretching exercises before you run or perform any activity that stresses the knee.
- Gradually increase training. Never abruptly increase the intensity of your workout. Instead, make changes incrementally.
- Use proper running shoes. Buy quality shoes with good shock absorption, and make sure they fit properly and comfortably. Don’t run in shoes that are too worn. Wear orthotics if you have flat feet.
- Use proper running form. Keep a tight core to prevent yourself from leaning too far forward or backward, and keep your knees bent. Try to run on a soft, smooth surface. Avoid running on concrete. Walk or run in a zigzag pattern when going down a steep incline.
HAMSTRING INJURY:
 A hamstring injury is a strain or tear to the tendons or large muscles at the back of the thigh.
A hamstring injury is a strain or tear to the tendons or large muscles at the back of the thigh.
It’s a common injury in athletes and can occur in different severities. The 3 grades of hamstring injury are:
- grade 1– a mild muscle pull or strain
- grade 2– a partial muscle tear
- grade 3– a complete muscle tear
The length of time it takes to recover from a hamstring strain or tear will depend on how severe the injury is.
A minor muscle pull or strain (grade 1) may take a few days to heal, whereas it could take weeks or months to recover from a muscle tear (grade 2 or 3).
The hamstrings
The hamstrings are tendons (strong bands of tissue) at the back of the thighs that attach the large thigh muscle to the bone.
The term “hamstring” also refers to the group of 3 muscles that run along the back of your thigh, from your hip to just below your knee.
The hamstring muscles are not used much while standing or walking, but they’re very active during activities that involve bending the knee, such as running, jumping and climbing.
Causes:
A hamstring injury can occur if any of the tendons or muscles are stretched beyond their limit.
They often occur during sudden, explosive movements, such as sprinting, lunging or jumping. But they can also occur more gradually, or during slower movements that overstretch your hamstring.
Recurring injury is common in athletes and sportsmen, as you’re more likely to injure your hamstring if you’ve injured it before.
Symptoms:
Partial hamstring tears (grade 2) are usually more painful and tender. swelling and bruising at the back of your thigh loss of strength .
Severe hamstring tears (grade 3) will usually be very painful, tender, swollen and bruised. There may have been a “popping” sensation at the time of the injury and you’ll be unable to use the affected leg.
Diagnosis: USG / MRI
TREATMENT:
Recovering from a hamstring injury may take days, weeks or months, depending on how severe it is.
A completely torn hamstring may take several months to heal and you’ll be unable to resume training or play sport during this time.
Initial treatment
During the first 2 or 3 days, you should care for your injury using RICE therapy:
- Rest – keep your leg as still as you possibly can and avoid physical activity. Your GP may recommend using crutches in more severe cases.
- Ice – apply cold packs (a bag of frozen peas wrapped in a tea towel will also work) to your hamstring for up to 20 minutes every 2 to 3 hours during the day. Do not apply ice directly to your skin.
- Compression – compress or bandage the thigh to limit any swelling and movement that could cause further damage. You can use a simple elastic bandage or elasticated tubular bandage available from a pharmacy.
- Elevation – keep your leg raised and supported on a pillow as much as possible, to help reduce any swelling.
Regular painkillers, such as paracetamol or a non-steroidal anti-inflammatory drug (NSAID) cream or gel, may also help relieve the pain.
Gentle exercises and stretches
Returning to strenuous exercise too quickly could make your injury worse, but avoiding exercise for too long can cause your hamstring muscles to shrink and scar tissue to form around the tear.
To avoid this, you should start doing gentle hamstring stretches after a few days, when the pain has started to subside.
This should be followed by a programme of gentle exercise, such as walking and cycling, and hamstring strengthening exercises.
To avoid injuring yourself again, you should only return to a full level of activity when your hamstring muscles are strong enough.
ASPIRATION OF HEMATONA: If swelling is too big
PRP Injections: it provides high concentrate of growth factors helps in speedy recovery
Surgery: very rare but in grade three injuries
QUADRICEPS INJURY:
 It consists of four individual muscles; three vastus muscles and the rectus femoris. They form the main bulk of the thigh, and collectively are one of the most powerful muscles in the body. It is located in the anterior compartment of the thigh.
It consists of four individual muscles; three vastus muscles and the rectus femoris. They form the main bulk of the thigh, and collectively are one of the most powerful muscles in the body. It is located in the anterior compartment of the thigh.
Functions: helps in knee extension and hip flexion
Cause:
- Sudden contraction of muscles
- Trauma
Symptoms: pain, selling, contusion and unable to extend the knee
Diagnosis: clinical / usg / Mri
Treatment:
- RICE
- NSAIDS
- Physiotherapy : Stretching Exercises
- Strengthening
- Sports Specific Rehabilitation
- PRP Injections
- In Severe (Complete) Injuries : Surgery





