- Defined as a collective term that refers to movement of the scapula that is dysfunctional and may create a possible impairment of overall shoulder function
- Loss of control of normal scapular motion, physiology or mechanics
- Good scapula control and positioning
- optimal positioning of the humerus in relation to the glenoid and Transferring power from the core to the distal upper extremity
Scapular Dyskinesis
INTRODUCTION

Anatomy and Biomechanics
Skeletal Attachment:
- AC joint & GH joint
- Sternoclavicular joint
Muscles
- Trapizius
- Serratus anterior
- Rhomboid muscles
- Levator scapulae
- Cuff muscles
- Pec. Minor and short head of biceps
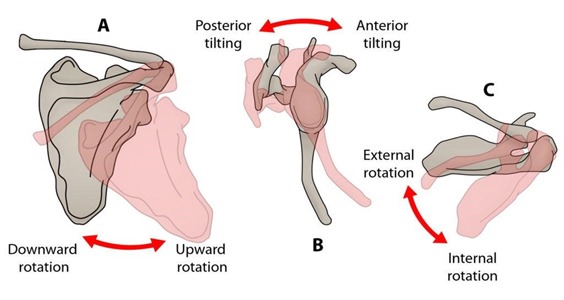
Movements:
- Upward/downward rotation around a horizontal axis perpendicular to the plane of the scapula
- Internal/external rotation around vertical axis through the plane of the scapula
- Anterior/posterior tilt around a horizontal axis in the plane of the scapula
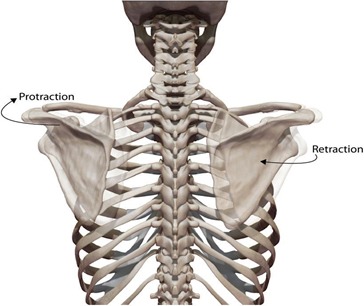
Coupling Movements of Scapula
- Retraction : external rotation, posterior tilt, upward rotation and medial translation
- Protraction : internal rotation, anterior tilt, downward rotation and lateral translation
- Shrug : upward translation, anterior tilt and internal rotation
- Coupling movements maintain glenoid as congruent socket, maximizing concavity compression and kinematics
- Scapula stabilized in retraction posture during arm elevation to achieve maximal activation of all muscles originating on the scapula
Stability and Mobility
- The clavicle acts as a strut
- This allows two translations to occur—upward/downward translation on the thoracic wall and retraction/protraction around the rounded thorax.
- When the humerus moves into elevation, clavicular elevation, retraction and posterior axial rotation occur at the sternoclavicular joint.
- while scapular internal rotation, upward rotation and posterior tilting occur at the acromioclavicular joint.
- AC joint – scapular posterior tilt.
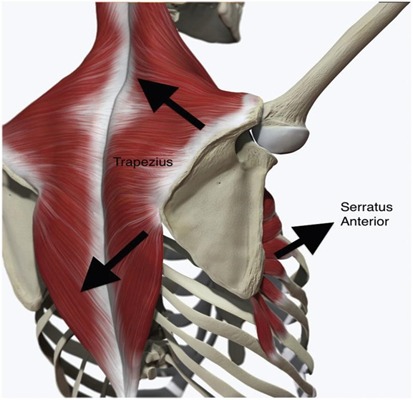
- The upper and lower trapezius muscles in addition to the serratus anterior muscles have been shown to be the greatest contributors to scapular stability and mobility.
- The trapezius and serratus anterior muscle initiate upward rotation and posterior tilt of the scapula.
- Activation of the lower trapezius muscle plays an important role in the stability of the arm in the overhead position and in descent of the arm from a position of maximum elevation.
- The rhomboids assist the trapezius in stabilizing the scapula contributing to control of medial and lateral scapular translation.
- Latissimus dorsi and pectoralis minor : prime mover of arm.
Force couples:
- For scapular stabilization :
upper/ lower trapezius + serratus anterior paired with Rhomboid muscles
- For acromial elevation : lower trapezius + serratus anterior
paired with upper trapezius + rhomboid
At early movement
The upper and lower trapezius and serratus anterior muscles have long lever arms, being effective rotators and stabilizers.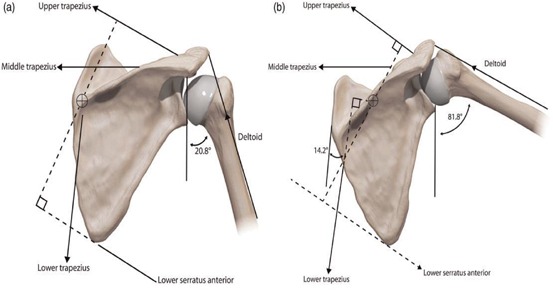
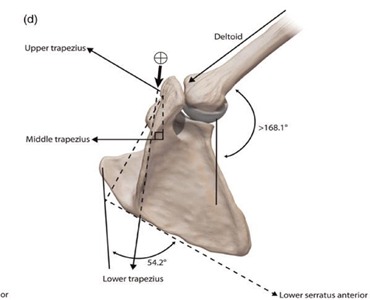
- With higher arm elevation the upper trapezius moment arm is shorter, whereas the lower trapezius and serratus anterior moment arms remain long, continuing to rotate the scapula
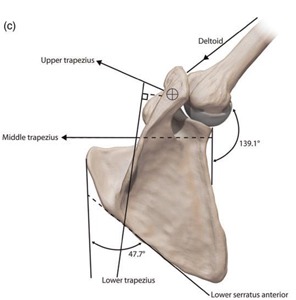
- With maximum arm elevation, the lower trapezius maintains scapula position and the instant centre of rotation moves from the medial border of the spine to the acromioclavicular joint
- The levator scapulae functions to elevate the scapula and tilt the glenoid cavity inferiorly by rotating the scapula downward
Clinical features:
- Static : asymmetry prominence of scapulae resting position of protraction
- Dynamic :
- medial border prominence
- inferior angle prominence and/or early scapular elevation or shrugging on arm elevation
- rapid downward rotation during arm lowering
- Tenderness over coracoid
Causes:
- Bony : thoracic kyphosis
clavicle fractures – malunion shortening rotation
JSES,2015

Scapular dyskinesis is common after displaced middle-third clavicle fractures and these patients have more pain and worse functional outcomes compared with patients without scapular dyskinesis.
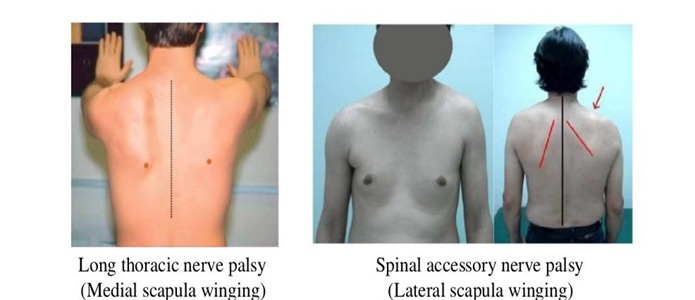
Neurological
- Long thoracic nerve – serratus anterior
- Spinal accessory nerve – trapezius
- Cervical radiculopathy
 Dorsal scapular nerve – rhomboid
Dorsal scapular nerve – rhomboid
 Soft Tissue Causes
Soft Tissue Causes
- Intrinsic muscle pathology
- Inhibition of normal muscle activation – commonly lower trapezius and serratus anterior
- Inflexibility : decreased flexibility in pec.minor, short head biceps causes traction through coracoid
- Anterior tilt and internal rotation – protraction
JSES,2018
- In the intervention limb group, the shoulder was passively and horizontally abducted at 150° of elevation for 5 minutes to stretch the pectoralis minor muscle
- Stretching for the pectoralis minor muscle increases external rotation and posterior tilt of the scapula during arm elevation

JOINT RELATED :
- AC joint dislocations : acromion displaced medially and inferiorly
- Leads to anterior tilt , internal rotation and loss of upward rotation – protraction scapula
- JOAS,2009 : Chronic type III AC dislocation causes scapular dyskinesis in 70.6% of patients. Of the latter, 58.3% have SICK scapula syndrome developed.
LATARJET
JSES,2015
- Scapular dyskinesis was found in 5 of 20 patients who underwent a Latarjet procedure.
- Dyskinesis may be related to the detachment of the pectoralis minor, and variation of the vector and the working length of the coracobrachialis and the short head of the biceps.

Clinical Evaluation
 Observation of static scapular position – rest , hands on both hips and 90deg abduction with full internal rotation
Observation of static scapular position – rest , hands on both hips and 90deg abduction with full internal rotation- Observation of scapular motion –
- Kibler’s four-type rating system, which required a single-forced choice among four categories, including three subtypes of dyskinesis: types
- I (inferior angle prominence),
- II (medial border prominence),
- III (excessive superior border elevation) and
- IV (symmetric and normal scapular motion).
- More specifically, weighted flexion was the motion that most commonly resulted in dyskinesis and a 3-kg load significantly reduced scapulothoracic motion through the range of 35°–45° of glenohumeral motion.
Scapula assistance test
- Scapula assistance test: the scapula is stabilized with one hand and the other hand ‘assists’ the scapula through its correct motion plane.
- The SAT evaluates scapular contributions to impingement and rotator cuff strength
- This procedure simulates the force-couple activity of the serratus anterior and lower trapezius muscles

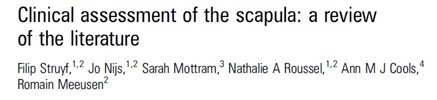
Scapular retraction test
- Scapula retraction test: the examiner stabilizes the medial border of the scapula as the arm is elevated. Relief of impingement symptoms is a positive test.
- The SRT can be used for evaluation in cases of labral symptoms and rotator cuff strength.

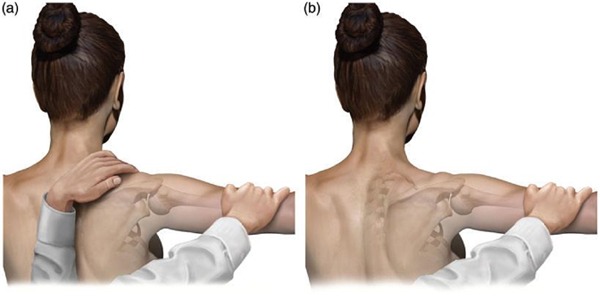
Lateral scapular slide test
- Quantitative assessment of scapular stabilizer strength
- Lateral scapula slide test. (a) Initial position with arm at side. (b) Second position, arms on hips. (c) Third position with arms at 90 and internal rotation
- The threshold of abnormality is 1.5 cm and significant asymmetry is most commonly measured in the third position.

Scapula retraction test with resistance
• (a) The examiner performs a traditional ‘empty can’ test.
• (b) The examiner stabilizes the medial border of the scapula and repeats the test. If the impingement symptoms are relieved, the test is positive
Other tests
- Baylor square and double-square technique
- Measurement of the distance between the posterior border of the acromion and the table/wall
- Measurement of the pectoralis minor muscle length
- Measurement of scapular upward rotation
Other investigations
- X ray
- EMG/NCVS
- Mri shoulder and c spine
Treatment :
Physical therapy
- To relieve the symptoms associated with inflexibility or trigger points and to re-establish muscle strength and activation patterns
- Surgery physiotherapy in Dyskinesis can often be caused by muscle inhibition created by soft tissue related pathology such as labral injury, internal impingement or rotator cuff pathology or hard tissue injury such as clavicle fractures and AC separations.
- Rehabilitation for scapular dyskinesis should start proximally and end distally.
- Core muscle strengthening : which the larger muscles of the lower extremity and trunk are utilized during the treatment of the scapula and shoulder
- Scapular protraction and retraction are facilitated by hip and trunk flexion and extension exercises.
- Lower trapezius and serratus strengthening (short lever, kinetic chain assisted exercises and finally long lever movements)
- Rotator cuff strengthening
References



- Scapular Dyskinesis and Its Relation to Shoulder Injury, JAAOS,2012

Q&As on Scapular Dyskinesis
What Is Scapular Dyskinesis?
The scapula (shoulder blade) needs support for the rotator cuff to contract and function properly, andthe scapula must rotate. Any soft tissue or bone damage around the shoulder may change the scapula’s functions while in motion or at rest. A change or departure from the scapula’s typical resting or active posture during shoulder movement is known as scapular dyskinesis (also known as SICK scapula). Since most individuals use their shoulders repeatedly, the scapula often moves abnormally. These alterations may raise the risk of harm even if they are sometimes asymptomatic.
What Are the Symptoms of Scapular Dyskinesis?
Symptoms of scapular dyskinesis are:
- Experiencing pain and soreness around the scapula while lifting above heavy goods with the affected arm or while using the affected arm to carry heavy objects..
- Experiencing a popping or snapping feeling around the scapula whenever the shoulder is moved
- A weakening of the muscles caused by repeated usage of the shoulder and arm.
- Affected side sitting lower that usual in a lopsided position.
- Positioning of the scapula in a winging position
- It feels like your shoulder is constantly shifting and dislocating due to instability.
How is Scapular Dyskinesis Diagnosed?
Typically, a diagnosis doesn’t require an MRI or x-ray. Doctors generally identify the condition based on a physical checkup, they may also look for physical indicators of prior injuries that may have contributed to the dysfunction in your shoulder. In some instances, a specific nerve test is utilised to assess the severity of your injury and establish the best course of action.
Consider mentioning it if you find that a specific activity exacerbates your pain or discomfort. Include information about what occurred when you first noticed a loss of mobility or a change in the position of your shoulder blades.
How to Prevent Scapular Dyskinesis?
The following measures may help avoid scapular dyskinesis:
- Stretch and warm up before you throw or do any other overhead activity.
- You must meet specific pitch count and age criteria to play a sport.
- The right way to throw should be taught and practised from a young age.
- Paying attention to the right way to throw is especially important for young kids just starting to play sports.
- Don’t force a range of motion, especially when lifting.
How Is Scapular Dyskinesis Treated Non-surgically?
Stretches and strength exercises are utilised as the first line of therapy, along with medications and cold packs to reduce discomfort. The activity that first triggered the issue is also avoided or altered. Following the diagnosis, it might be essential to take some time off to give the shoulder a chance to rest. A physical therapist or sports trainer may often be suggested.
Ibuprofen and other non-steroidal anti-inflammatory drugs are often suggested. Take them as your doctor has prescribed. Call your doctor immediately if you face any bleeding, stomach discomfort, or symptoms of an allergic reaction.
Cold help reduce inflammation and discomfort; ce packs and massages help. After the injury, apply an ice pack for 15 minutes every 3 hours. Apply heat packs before specified stretches and strength exercises.
© Copyright 2025 Bangalore Shoulder Institute