There can be a number of reasons for the nerve entrapment especially at the suprascapular and spinoglenoid notches where nerve deviation is limited by bony and ligamentous structures. Additional compression may result due to ganglion cysts related to glenohumeral joint. In elderly people, suprascapular neuropathy occurs as a result of large rotator cuff tear.
Sports like tennis where frequent overhead positioning of the arm is required may cause suprascapular neuropathy. The exact location of the nerve entrapment determines whether supraspinatus as well as infraspinatus muscles are involved or just the infraspinatus muscle is involved. It cannot be said that sporting activities alone is the main cause of suprascapular neuropathy, direct trauma to the arm such as when falling on to the arm or other overuse type activities may also result in suprascapular neuropathy. Some surgical procedures of the shoulders may also damage the suprascapular nerve like a Bankart Repair where there is a high probability of suprascapular nerve injury. There are instances of suprascapular neuropathy in people who have undergone spinal surgery as a result of their positioning.
Symptoms
Burning and aching pain on the back and side of the shoulders are the primary symptoms of suprascapular neuropathy. The onset of the pain can be either spontaneous or gradual and will be deep set in the shoulders. The pain also radiates to the arms. Weakness of the shoulders when lifting things is another symptom experienced by people affected with this condition. As time goes by, wasting of the supraspinatus and infraspinatus muscles can also be noticed.
Diagnosis

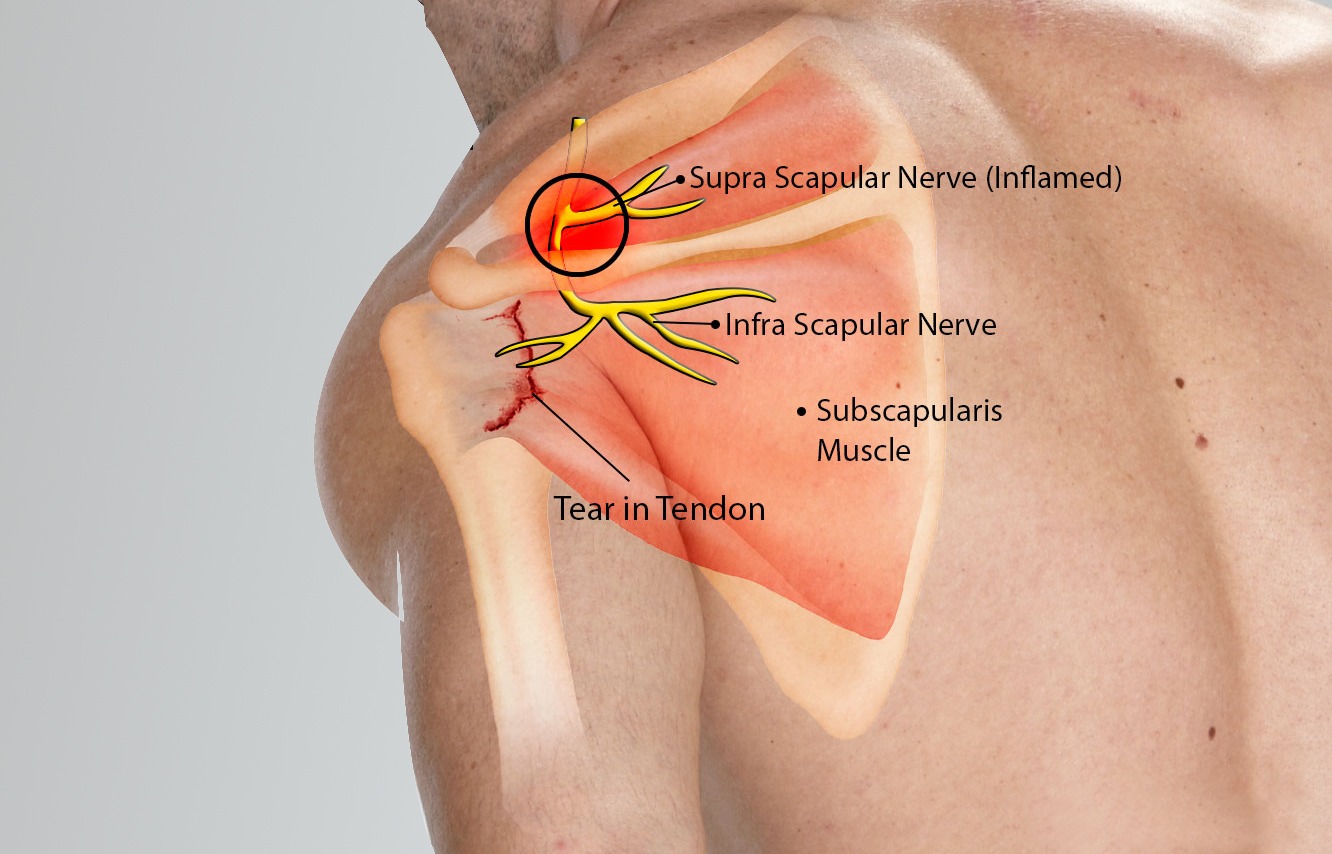
Patient presentation with supra scapular nerve palsy
Significant nerve muscle atrophy/wasting
If suprascapular neuropathy is suspected, the first line of action is to get a radiological study to have a detailed look at the structures. Along with standard views, the suprascapular notch and Stryker views are also taken. Unless there is a trauma to account for this condition, radiographic findings are usually unremarkable. Apart from x-rays, MRI of the shoulder may also be required to see if there is muscle edema along with muscle atrophy. An MRI may also throw light on the presence of a ganglion cyst with resultant compression of the suprascapular nerve.
Another important tool to diagnose suprascapular neuropathy is 3T magnetic resonance, as it identifies nerve abnormalities or denervation changes in the muscles. Being an affordable option, ultrasound is also an important diagnostic tool in identifying suprascapular neuropathy. Ultrasound also has the capability to give precise information.
Apart from the above-mentioned tests, electrodiagnostic study is also very helpful in assessing suprascapular neuropathy. EMG may reveal positive sharp waves and fibrillation potentials suggestive of denervation. There may also be motor unit recruitment abnormalities observed during the study.
Treatment
There are mainly three ways through which scapular neuropathy can be treated viz. conservative measures, surgical procedures and nerve blocks for which studies have shown to be quite beneficial.
Conservative measures:
In cases where suprascapular neuropathy does not give rise to pain or limitation of activity then physical therapy exercises in the form of scapular stabilization and mobilization is enough for relieving symptoms if any and resolving the condition. Treatment may take about a month to finish. This exercise programme is planned in such a way to stem further progression of the disease condition. Impingement of the rotator cuff can also be prevented through this exercise regimen. Physical therapy is recommended when a person is showing the tell-tale signs of scapular neuropathy. Exercise programme is designed to improve flexibility and stability of the shoulders. It should also be noted that in addition to an exercise programme, modification of activities also becomes imperative by way of limiting the amount of work they do, especially during the acute phase of the disease.
Surgical measures:
If conservative measures fail to give the desired result, then the next line of treatment is surgical approach to treat the condition. Surgical procedure is designed in such a way to free up the space for the nerve by widening of the suprascapular or the supraglenoid notch depending on where the nerve is getting compressed.
Arthroscopic surgery:

Arthroscopic picture of Supra Scapular Nerve release
The instrument is probing the nerve
Arthroscopic approach (keyhole) is a more accurate method of approached suprascapular nerve entrapment. Arthroscopic release of the entrapped scapular nerve can be performed safely and effectively. Being a minimally invasive procedure, this surgery is gaining a lot of ground of late. It is done by inserting an endoscope (a flexible tube with a light and camera attached to it) into the joint through a small incision. As there is direct vision of the medial neck of the glenoid, complications during the surgery can be reduced to a minimum. Post surgery most of the patients have reported marked improvement in pain relief and function.
Nerve blocks:
In addition to conservative and surgical approaches, nerve blocks can also be used to treat suprascapular neuropathy. These blocks provide significant relief of symptoms by anesthetizing (numbing) the suprascapular nerve with an injection, relieving the shoulder pain arising out of this condition.
For enquiries and online appointments, send message to www.BangaloreShoulderInstitute.com/contact