- By shoulderadm
- In Shoulder
Treatment of Irreparable Rotator Cuff Tears Using Superior Capsular Reconstruction (SCR)
Rotator cuff tears are a common ailment, causing pain and limiting movement for many. While most can be effectively managed with physiotherapy and, if necessary, surgical repair, some tears are simply too large or too damaged to be fixed using traditional methods. These “irreparable” tears pose a significant challenge for both patients and orthopaedic surgeons. Fortunately, advancements in surgical techniques are offering new hope, and one such promising innovation is Superior Capsular Reconstruction or SCR.
What is Superior Capsular Reconstruction (SCR)?
Superior Capsular Reconstruction (SCR) is a surgical technique aimed at rebuilding the upper portion of the shoulder joint’s lining, known as the superior capsule. The procedure involves anchoring tissue from the glenoid (shoulder socket) to the greater tuberosity (upper part of the humerus), effectively strengthening the superior capsule. This bolstering action helps to keep the head of the humerus properly positioned within the glenoid, counteracting the instability that results from a compromised rotator cuff. The surgery accomplishes this reconstruction using either tissue taken from the patient’s own body (autograft) or tissue sourced from a donor (allograft).
How SCR Improves Shoulder Function
The SCR technique counteracts the loss of support caused by a deficient rotator cuff by rebuilding the superior capsule, which is crucial for proper joint mechanics. This procedure aims to:
- Stabilise the Shoulder: The reconstructed capsule helps maintain the correct positioning of the humeral head within the glenoid socket.
- Reduce Pain: Restoring stability and proper mechanics can alleviate pain associated with rotator cuff deficiency.
- Enhance Function: Patients may experience an improved range of motion and overall shoulder function following SCR.
The SCR Procedure
Typically performed arthroscopically, SCR involves using a small camera (arthroscope) to visualise the shoulder joint. This allows the surgeon to assess damage and perform the reconstruction through small incisions. Here’s a general overview of the steps:
- Patient Positioning and Anesthesia: The patient is positioned, and regional and/or general anaesthesia is administered.
- Arthroscopic Access: Small incisions are made to insert the arthroscope and specialised surgical instruments.
- Joint Assessment and Preparation: The shoulder joint is examined, and any necessary debridement or partial rotator cuff repair is performed.
- Bone Preparation: The bone surfaces on the glenoid (socket) and humerus (upper arm bone) are prepared to receive the graft.
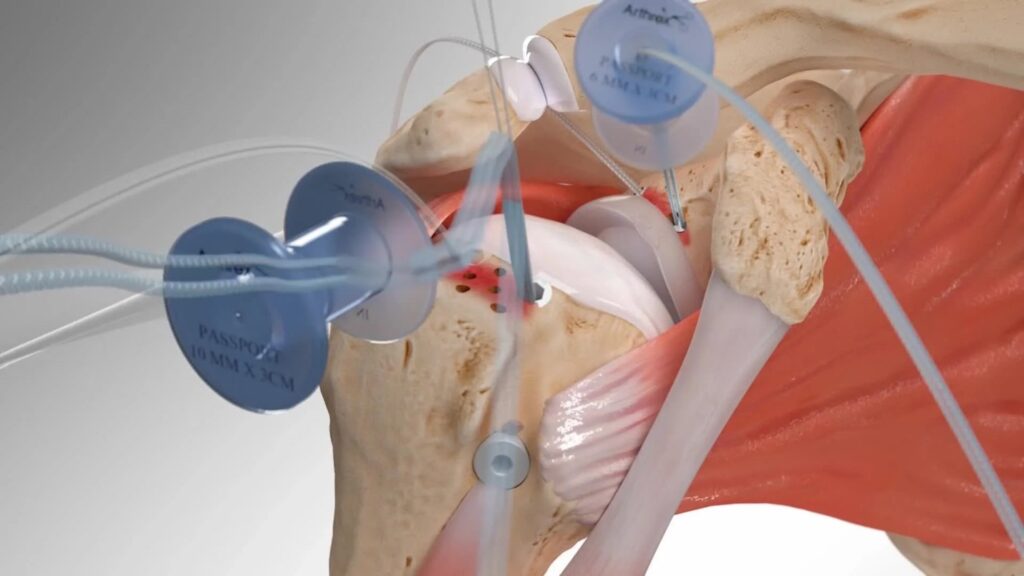
- Anchor Placement: Suture anchors are inserted into the bone to secure the graft.
- Graft Placement and Fixation: A strong graft, often a porcine graft, is passed into the joint and secured to the prepared bone using the previously placed sutures. The surgeon ensures the graft is well-secured to the humeral head.
- Graft Securement: The suture strands are further secured by lateral anchors (double-row technique). The peripheral edges of the graft (anteriorly and posteriorly) are secured to the native remnant tissue to relink the construct.
- Final Assessment and Closure: The surgeon performs a final evaluation of the reconstruction and closes the incisions.
Conclusion
Following SCR, the shoulder is immobilised in a sling for approximately six weeks, with physiotherapy guiding recovery. It presents a viable surgical option for suitable patients seeking improved shoulder biomechanics and pain reduction, potentially enabling a return to higher levels of activity.
For enquiries and online appointments, send a message to www.BangaloreShoulderInstitute.com/contact
For informative videos related to Shoulder problems and their treatment options, Sports Injuries and other orthopedic conditions, visit the YouTube channel Bangalore Shoulder Institute – https://www.youtube.com/@BangaloreShoulderInstitute




